News release
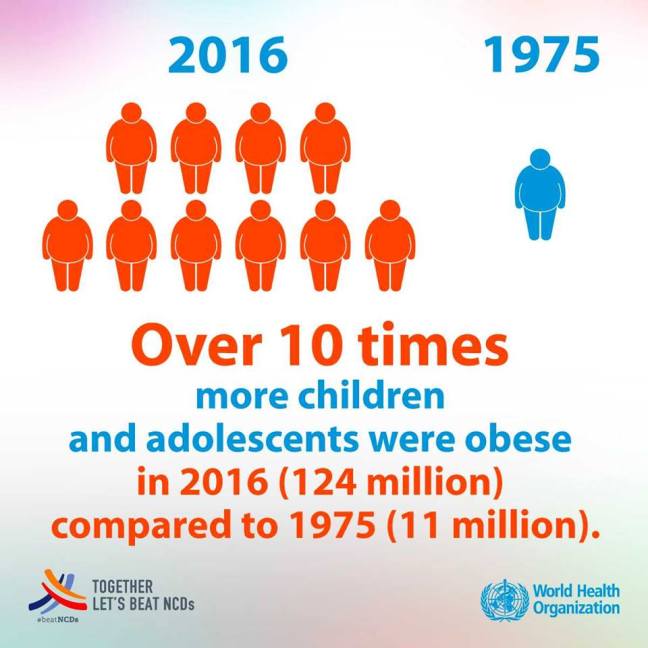
11 OCTOBER 2017 | LONDON – The number of obese children and adolescents (aged five to 19 years) worldwide has risen tenfold in the past four decades. If current trends continue, more children and adolescents will be obese than moderately or severely underweight by 2022, according to a new study led by Imperial College London and WHO.
The study was published in The Lancet ahead of World Obesity Day (11 October). It analysed weight and height measurements from nearly 130 million people aged over five years (31.5 million people aged five to 19, and 97.4 million aged 20 and older), making it the largest ever number of participants involved in an epidemiological study. More than 1000 contributors participated in the study, which looked at body mass index (BMI) and how obesity has changed worldwide from 1975 to 2016.
Obesity rates in the world’s children and adolescents increased from less than 1% (equivalent to five million girls and six million boys) in 1975 to nearly 6% in girls (50 million) and nearly 8% in boys (74 million) in 2016. Combined, the number of obese five to 19 year olds rose more than tenfold globally, from 11 million in 1975 to 124 million in 2016. An additional 213 million were overweight in 2016 but fell below the threshold for obesity.
Food marketing, policies, pricing behind obesity rise
Lead author Professor Majid Ezzati, of Imperial’s School of Public Health, says: “Over the past four decades, obesity rates in children and adolescents have soared globally, and continue to do so in low- and middle-income countries. More recently, they have plateaued in higher income countries, although obesity levels remain unacceptably high.”
Professor Ezzati adds: « These worrying trends reflect the impact of food marketing and policies across the globe, with healthy nutritious foods too expensive for poor families and communities. The trend predicts a generation of children and adolescents growing up obese and at greater risk of diseases, like diabetes. We need ways to make healthy, nutritious food more available at home and school, especially in poor families and communities, and regulations and taxes to protect children from unhealthy foods. »
More obese than underweight 5 to 19 year olds by 2022 but underweight persists in poor regions
The authors say that if post-2000 trends continue, global levels of child and adolescent obesity will surpass those for moderately and severely underweight youth from the same age group by 2022. In 2016, the global number of moderately or severely underweight girls and boys was 75 million and 117 million respectively.
Nevertheless, the large number of moderately or severely underweight children and  adolescents in 2016 (75 million girls and 117 million boys) still represents a major public health challenge, especially in the poorest parts of the world. This reflects the threat posed by malnutrition in all its forms, with there being underweight and overweight young people living in the same communities.
adolescents in 2016 (75 million girls and 117 million boys) still represents a major public health challenge, especially in the poorest parts of the world. This reflects the threat posed by malnutrition in all its forms, with there being underweight and overweight young people living in the same communities.
Children and adolescents have rapidly transitioned from mostly underweight to mostly overweight in many middle-income countries, including in East Asia, Latin America and the Caribbean. The authors say this could reflect an increase in the consumption of energy-dense foods, especially highly processed carbohydrates, which lead to weight gain and poor lifelong health outcomes.
Dr Fiona Bull, programme coordinator for surveillance and population-based prevention of noncommunicable diseases (NCDs) at WHO, says: “These data highlight, remind and reinforce that overweight and obesity is a global health crisis today, and threatens to worsen in coming years unless we start taking drastic action.”
Solutions exist to reduce child and adolescent obesity
In conjunction with the release on the new obesity estimates, WHO is publishing a summary of the Ending Childhood Obesity (ECHO) Implementation Plan. The plan gives countries clear guidance on effective actions to curb childhood and adolescent obesity. WHO has also released guidelines calling on frontline healthcare workers to actively identify and manage children who are overweight or obese.
Dr Bull adds: “WHO encourages countries to implement efforts to address the environments that today are increasing our children’s chance of obesity. Countries should aim particularly to reduce consumption of cheap, ultra-processed, calorie dense, nutrient poor foods. They should also reduce the time children spend on screen-based and sedentary leisure activities by promoting greater participation in physical activity through active recreation and sports.”
Note for Editors:
The paper presents the first ever comprehensive data on underweight through to obesity for children and adolescents aged five to 19 years and provides startling findings on the increasing numbers and rates of young people being affected by obesity.
The study calculated and compared body mass index (BMI) among children, adolescents and adults from 1975 to 2016, and made projections based on current trends in obesity rates.
BMI is a measure of a person’s weight and body fat mass for their height, and indicates whether their weight is healthy.
Calculating BMI is the simplest way to assess a person’s weight status, and the most common tool used to determine under-, healthy- and overweight and obesity. For children and adolescents, their BMI is adjusted for age and sex using WHO’s growth reference curves.
Action to curb obesity is a key element of the 2030 Agenda for Sustainable Development. Sustainable Development Goal (SDG) target 3.4 commits the world to reducing premature deaths from NCDs by one-third by 2030, including through prevention of obesity. SDG target 2.2 commits the world to ending all forms of malnutrition by 2030, including overweight and obesity. Also, the goal of the United Nations Decade of Action on Nutrition (2016-2025) is to promote collaboration across all sectors and stakeholders to end malnutrition in all its forms.
The findings also showed that:
Global data for obesity and underweight
In 2016, there were 50 million girls and 74 million boys with obesity in the world, while the global number of moderately or severely underweight girls and boys was 75 million and 117 million respectively.
The number of obese adults increased from 100 million in 1975 (69 million women, 31 million men) to 671 million in 2016 (390 million women, 281 million men). Another 1.3 billion adults were overweight, but fell below the threshold for obesity.
Regional/Country data for obesity, BMI and underweight
Obesity:
The rise in childhood and adolescent obesity rates in low and middle income countries, especially in Asia, has recently accelerated. On the other hand, the rise in childhood and adolescent obesity in high income countries has slowed and plateaued.
In 2016, the obesity rate was highest in Polynesia and Micronesia in boys and girls, at 25.4% in girls and 22.4% in boys, followed by the high-income English-speaking region, which includes the USA, Canada, Australia, New Zealand, Ireland and the United Kingdom.
The areas of the world with the largest increase in the number of obese children and adolescents were East Asia, the high-income English-speaking region, and the Middle East and North Africa.
Nauru was the country with the highest prevalence of obesity for girls (33.4%), and Cook Islands had the highest for boys (33.3%).
In Europe, girls in Malta and boys in Greece had the highest obesity rates, comprising 11.3% and 16.7% of the population respectively. Girls and boys in Moldova had the lowest obesity rates, comprising 3.2% and 5% of the population respectively.
Girls in the UK had the 73rd highest obesity rate in the world (6th in Europe); boys had the 84th highest obesity in the world (18th in Europe).
Girls in the USA had the 15th highest obesity rate in the world; boys had the 12th highest obesity in the world.
Among high-income countries, the United States of America had the highest obesity rates for girls and boys.
BMI:
The largest rise in BMI of children and adolescents during the four decades was in Polynesia and Micronesia for both boys and girls, and in central Latin America for girls. The smallest rise in the BMI of children and adolescents during the four decades covered by the study was seen in Eastern Europe.
The country with the biggest rise in BMI for girls was Samoa, which rose by 5.6 kg/m2, and for boys was the Cook Islands, which rose by 4.4 kg/m2.
Underweight:
India had the highest prevalence of moderate and severe underweight throughout these four decades (24.4% of girls and 39.3% of boys were moderately or severely underweight in 1975, and 22.7% and 30.7% in 2016). 97 million of the world’s moderately or severely underweight children and adolescents lived in India in 2016.
28 SEPTEMBER 2017 | GENEVA – Worldwide, 25 million unsafe abortions (45% of all abortions) occurred every year between 2010 and 2014, according to a new study by WHO and the Guttmacher Institute published today in The Lancet. The majority of unsafe abortions, or 97%, occurred in developing countries in Africa, Asia and Latin America.
“Increased efforts are needed, especially in developing regions, to ensure access to contraception and safe abortion,” says Dr Bela Ganatra, lead author of the study and a scientist in the WHO Department of Reproductive Health and Research.
“When women and girls cannot access effective contraception and safe abortion services, there are serious consequences for their own health and that of their families. This should not happen. But despite recent advances in technology and evidence, too many unsafe abortions still occur, and too many women continue to suffer and die.”
Classifying abortion safety
The new Lancet study provides estimates on safe and unsafe abortions globally. For the first time, it includes sub-classifications within the unsafe abortion category as less safe or least safe. The distinction allows for a more nuanced understanding of the different circumstances of abortions among women who are unable to access safe abortions from a trained provider.
When abortions are performed in accordance with WHO guidelines and standards, the risk of severe complications or death is negligible. Approximately 55% of all abortions from 2010 to 2014 were conducted safely, which means they were performed by a trained health worker using a WHO-recommended method appropriate to the pregnancy duration.
Almost one-third (31%) of abortions were “less safe,” meaning they were either performed by a trained provider using an unsafe or outdated method such as “sharp curettage”, or by an untrained person albeit using a safe method like misoprostol, a drug that can be used for many medical purposes, including to induce an abortion.
About 14% were “least safe” abortions provided by untrained persons using dangerous methods, such as introduction of foreign objects and use of herbal concoctions. Deaths from complications of unsafe abortion were high in regions where most abortions happened in the least safe circumstances. Complications from “least-safe” abortions can include incomplete abortion (failure to remove all of the pregnancy tissue from the uterus), haemorrhage, vaginal, cervical and uterine injury, and infections.
Restrictive laws associated with high rates of unsafe abortions
The study also looks at the contexts that commonly result in women seeking unsafe abortions, including countries’ laws and policies on abortion, the financial cost of accessing safe abortion services, the availability of safe abortion services and trained health providers, and societal attitudes toward abortion and gender equality.
In countries where abortion is completely banned or permitted only to save the woman’s life or preserve her physical health, only 1 in 4 abortions were safe; whereas, in countries where abortion is legal on broader grounds, nearly 9 in 10 abortions were done safely. Restricting access to abortions does not reduce the number of abortions.
Most abortions that take place in Western and Northern Europe and North America are safe. These regions also have some of the lowest abortion rates. Most countries in these regions also have relatively permissive laws on abortion; high levels of contraceptive use, economic development, and gender equality; as well as high-quality health services – all factors that contribute to making abortion safer.
“Like many other common medical procedures, abortion is very safe when done in accordance with recommended medical guidelines and that is important to bear in mind,” says Dr Gilda Sedgh, co-author of the study and principal research scientist, Guttmacher Institute.
“In the high-income countries of North America and Western and Northern Europe, where abortion is broadly legal and health systems are strong, the incidence of unsafe abortions is the lowest globally.”
Among developing regions, the proportion of abortions that were safe in Eastern Asia (including China) was similar to developed regions. In South-Central Asia, however, less than 1 in 2 abortions were safe. Outside of Southern Africa, less than 1 in 4 abortions in Africa were safe. Of those unsafe abortions, the majority were characterized as “least safe.”
In Latin America, only 1 in 4 abortions were safe, though the majority were categorized as “less safe,” as it is increasingly common for women in the region to obtain and self-administer medicines like misoprostol outside of formal health systems. This has meant that this region has seen fewer deaths and fewer severe complications from unsafe abortions. Nevertheless, this type of informal self-use of medication abortion that women have to resort to secretly does not meet WHO’s safe abortion standards.
Preventing unsafe abortion
Unsafe abortion occurs when a pregnancy is terminated either by persons lacking the necessary skills/information or in an environment that does not conform to minimal medical standards, or both.
To prevent unintended pregnancies and unsafe abortions, countries must make supportive policies and financial commitments to provide comprehensive sexuality education; a wide range of contraceptive methods, including emergency contraception; accurate family planning counselling; and access to safe, legal abortion.
Provision of safe, legal abortion is essential to fulfilling the global commitment to the Sustainable Development Goal of universal access to sexual and reproductive health (target 3.7). WHO provides global technical and policy guidance on the use of contraception to prevent unintended pregnancy, on safe abortion, and the treatment of complications from unsafe abortion.
Earlier this year, WHO and the Population Division of the United Nations Department of Economic and Social Affairs launched a new, open-access database of laws, policies and health standards on abortion in countries worldwide. The database aims to promote greater transparency of abortion laws and policies, as well as to improve countries’ accountability for the protection of women and girls’ health and human rights.
Mosquitoes are one of the deadliest animals in the world. Their ability to carry and spread disease causes millions of deaths every year.
If mosquitoes are around you, there are ways to protect yourself and your family.